

Introduction: Multiple myeloma (MM) is an incurable hematologic malignancy caused by the accelerated growth of clonal plasma cells. Daratumumab (dara) is a novel human monoclonal antibody that targets the CD38 transmembrane glycoprotein on the surface of plasma cells. Since its Food and Drug Administration approval, dara has been widely incorporated into clinical practice and has radically shifted the treatment paradigm of MM. The current study aimed to explore the pattern of use and overall outcomes when dara- based therapy is administered to patients with relapsed/refractory MM (RRMM) and newly-diagnosed MM (NDMM) in the real-world.
Methods: This retrospective study was conducted at a single institution and included patients with RRMM and NDMM who received dara-based therapy from 11/16/2015 to 3/16/2020. The study was approved by Institutional Review Board of Tufts Medical Center. Baseline demographics, clinical characteristics and therapy-related data were extracted from the electronic medical records. Hematologic responses were established based on IMWG criteria. Kaplan-Meier method was used to estimate survival data. Log-rank tests were applied to compare PFS among subgroups. Results were considered to be significant if two-sided P-value was less than or equal to 0.05. R software was used for statistics.
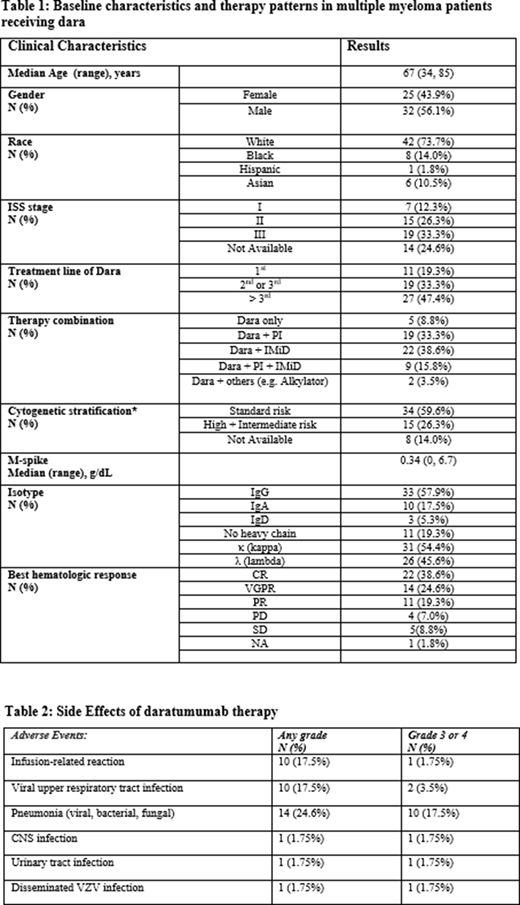
Results: Fifty-seven patients were included in the study. The median age was 67 years (range 34-85). Thirty-two patients (56.1%) were female and 42 (73.7%) were non-Hispanic White (Table 1). A third of patients had an International Staging System of III. By cytogenetic stratification, 34 (59.6%) of the participants had standard risk cytogenetics whereas 15 (26.3%) had high or intermediate risk cytogenetics. The vast majority of patients received dara at relapse (80.7%): 33.3% as 2/3rd line therapy and 47.4% as 4th line of therapy or higher. More than half (59.6%) of the subjects were stem cell transplant-naïve prior to the initiation of dara. Only 5 patients (8.8%) received dara monotherapy while 19 (33.3%) received dara + proteasome inhibitors (PI), 22 (38.6%) received dara + immunomodulator (IMiD), 9 (15.8%) received dara + PI + IMiD. The overall hematologic response rate was 82.5%, including 22 complete responses (CR) (38.6%), 14 very good partial responses (24.6%), and 11 partial responses (19.3%) (Table 1). The estimated median time to best hematologic response was 2.0 months (95% confidence interval [95% CI], 1.0, 2.5 months). Twenty-three (40.4%) of all subjects demonstrated disease progression during the follow-up period. The estimated median PFS for the entire cohort was 23.5 months ([95% CI], 12.2-not evaluable (NE)). When stratified by the treatment line (1st vs 2nd-3rd vs >3rd) and treatment pattern (dara monotherapy vs. combination with PI vs. IMiD vs. PI + IMiD), there were no significant differences of PFS between the aforementioned subgroups. However, subgroup analysis based on cytogenetic risks, demonstrated that patients with standard risk cytogenetics sustained a marginally significantly prolonged PFS (24.0 vs 10.0 months) compared to those with high/intermediate risk cytogenetics (p= 0.065). Dara was generally well tolerated without any instances of interruption or discontinuation. Ten individuals experienced infusion-related reactions that were mild-moderate and occurred during the first dara infusion only. The most common and serious (grade 3-4) infection was pneumonia. The major adverse events are highlighted in Table 2.
Conclusion: Dara-based therapy led to high and rapid overall response rates among the entire cohort. Our data suggest that patients with standard risk cytogenetics have improved outcomes from dara-based therapy in terms of progression free survival. These outcomes were superior to those who have high risk cytogenetics. Overall, this data justifies the widespread adoption of dara as part of a backbone therapy in MM.
Comenzo:Sanofi: Consultancy; Prothena: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Amgen: Consultancy; Unum: Consultancy; Caleum: Consultancy; Karyopharm: Consultancy, Research Funding; Janssen: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal